
Hypertrophic Cardiomyopathy (HCM) is a significant and often underdiagnosed cardiac condition, especially in younger populations.
A tragic case of a 17-year-old boy collapsing during a basketball game underscores the importance of understanding this condition.
Case Presentation
A 17-year-old boy, an active basketball player, suddenly collapsed during a game and was pronounced dead. The autopsy revealed an asymmetric hypertrophy of the interventricular septum. Upon microscopic examination, disorganized and thickened myofibrils with hyperchromatic nuclei were noted.
Overview of Hypertrophic Cardiomyopathy
Hypertrophic cardiomyopathy (HCM) is a genetic disorder characterized by the thickening (hypertrophy) of the heart muscle, primarily affecting the interventricular septum. The most common gene affected in the condition is a gene that codes for a protein called “myosin heavy chain (MHC)”. This protein plays a significant role in the contraction process of the myocardium. The inadequate contraction is compensated by the hypertrophy of the cardiomyocytes.
Hypertrophic cardiomyopathy is one of the most common inherited heart disorders, with an estimated prevalence of 1 in 500 people. It’s important to note that while HCM can occur at any age, it often goes undiagnosed because many people experience no symptoms and lead normal lives.
Pathophysiology
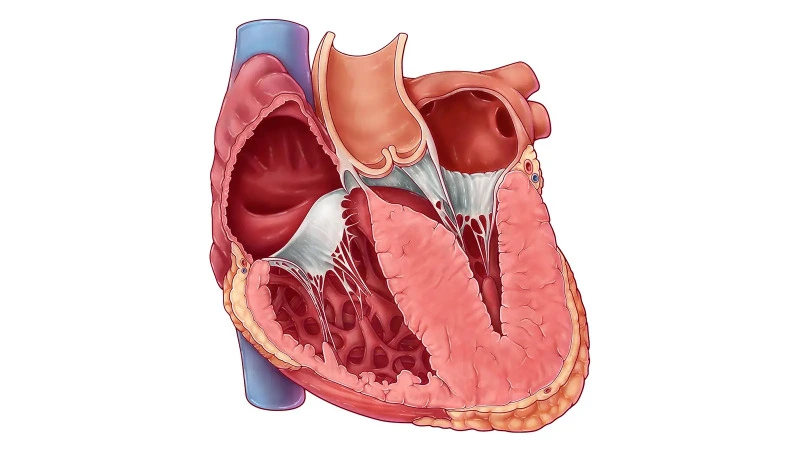
The hallmark of hypertrophic cardiomyopathy is asymmetric myocardial hypertrophy of the interventricular septum.
There are two reasons for decreased cardiac output in hypertrophic cardiomyopathy:
- The hypertrophy of the interventricular septum decreases the size of the left ventricle, thereby elevating the pressure required to fill it (elevated end-diastolic pressure). The filling of the left ventricle is impaired.
- The second reason is obstruction of the left ventricular outflow tract (LVOT) due to septal hypertrophy. Normally, the LVOT is a patent canal without any obstructions. However, when a septal myocardium obstructs the blood flow in the LVOT, cardiac output decreases and this type of HCM is called hypertrophic obstructive cardiomyopathy (HOCM). The high pressure gradient created by the obstruction of the LVOT pulls the anterior leaflet of the mitral valve towards the septum. This phenomenon, known as systolic anterior motion of the mitral valve, further exacerbates the obstruction of the LVOT.
On a microscopic level, the disorder is characterized by disorganized, thickened myofibrils and hyperchromatic nuclei.
Clinical Manifestations
Symptoms of HCM can vary widely among individuals. Some may be asymptomatic, while others might experience shortness of breath (dyspnea), chest pain (angina), palpitations, or fainting. Unfortunately, in some cases, such as the aforementioned incident, sudden cardiac death can be the first manifestation of the disease, especially in young athletes
Diagnosis
The diagnosis of HCM is primarily based on imaging, with echocardiography as the gold standard. It aids in visualizing the asymmetric enlargement of the interventricular septum.
Other diagnostic tools include electrocardiography (ECG), which may show signs of left ventricular hypertrophy, such as asymmetric T wave inversion in the lateral leads and voltage criteria for left ventricular hypertrophy; notably, 90% of patients with HCM have an abnormal ECG. MRI can be used to assess the extent of myocardial fibrosis. Genetic testing is also a consideration, particularly in cases with a family history of HCM.
Management and Treatment
Management of HCM is tailored to the individual’s symptoms and risk of complications. It includes lifestyle modifications, pharmacological treatment, and in some cases, surgical interventions.
Beta-blockers or calcium channel blockers are commonly used to manage symptoms and reduce the risk of sudden cardiac death. By controlling the heart rate, they prolong the diastole and enable the adequate filling process. Patients with HCM are often preload dependent, so they have to be adequately hydrated.
In symptomatic patients with obstructive HCM, surgical myectomy (the Morrow procedure) or alcohol septal ablation may be considered. Moreover, implantable cardioverter-defibrillators (ICDs) are recommended for patients at high risk of sudden cardiac death. The risk for the sudden cardiac death can be calculated here.
Preventive Strategies and Screening
Hypertrophic Cardiomyopathy, as highlighted by the case of the 17-year-old basketball player, is a complex and potentially deathly disease. Understanding its pathophysiology, clinical manifestations, diagnostic methods, and management strategies is of utmost importance for medical students.
Test your Knowledge on Hypertrophic Cardiomyopathy
Here is a brief quiz on the hypertrophic cardiomyopathy to assess your understanding of the material covered in this article.
